
Time Ladies and Gentlemen
A View from the Public Bar

Imagine the following scene: an airline pilot, a surgeon, or perhaps a schoolteacher, clearly intoxicated at work, stumbling through their duties. Before the day’s end, disciplinary proceedings would almost certainly be underway. Yet, within the Palace of Westminster, the same observation is so unremarkable that it has become woven into the fabric of the institution—a perk of power as old as the timbers of the building itself. As a Green MP recently remarked, “you can smell the alcohol when people are in between votes”, a comment that was met not with institutional reflection but with a barrage of criticism from colleagues who argued that the smell of “fags & beer” is simply what makes the place seem a “tiny bit normal”.
The debate over drinking in Parliament has flared once more, but it is not merely a question of etiquette or personal indulgence. It is a crisis of cognition, public health, and profound hypocrisy. The United Kingdom collectively spends billions managing the wreckage of alcohol-related harm—the most dangerous drug available—while simultaneously using public money to make it cheaper for the very people who legislate on its dangers. This article draws on clinical data, sociological research, and parliamentary records to expose the double standard at the heart of Westminster’s subsidised drinking culture.
The Bar Stool of Power
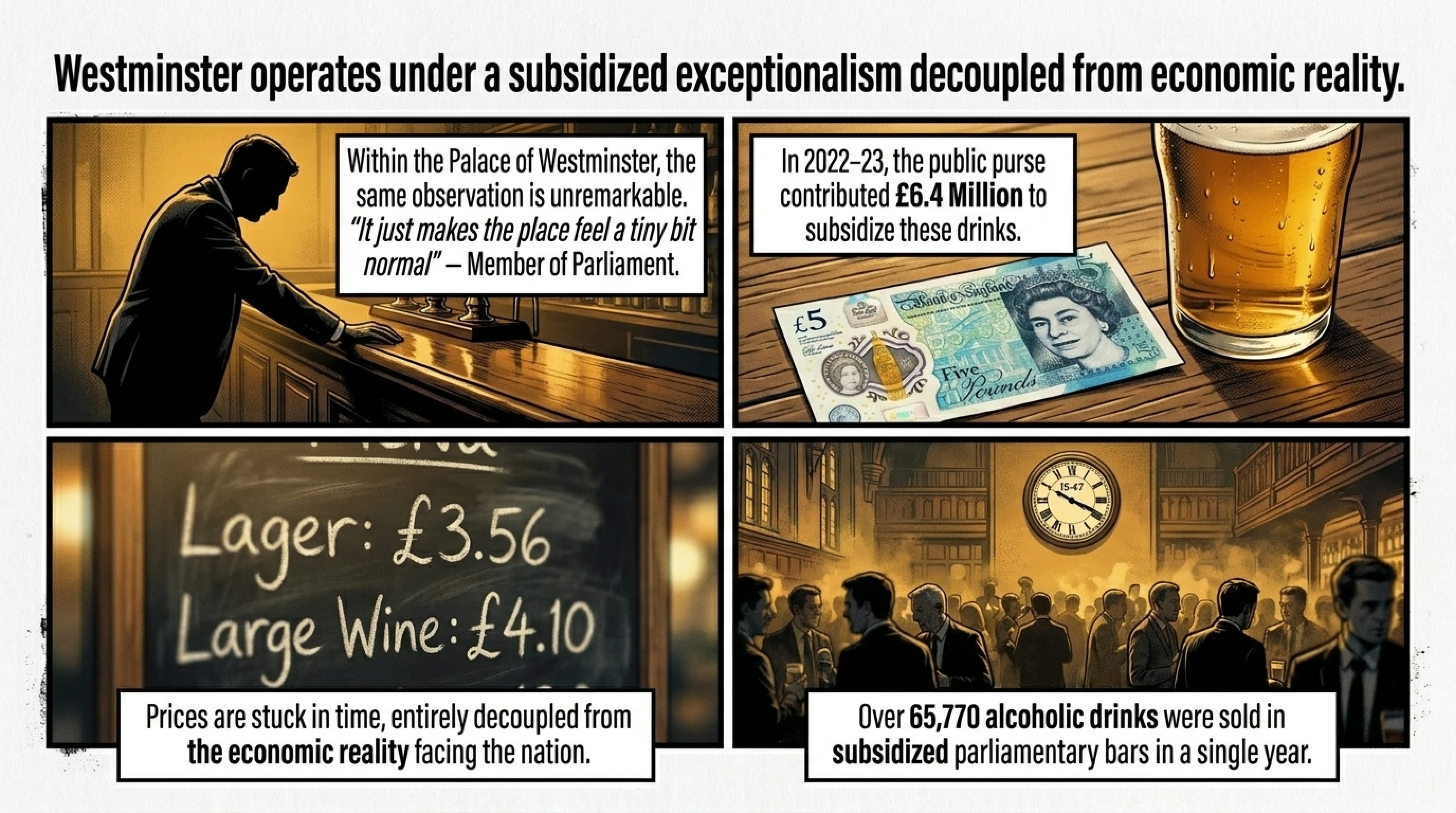
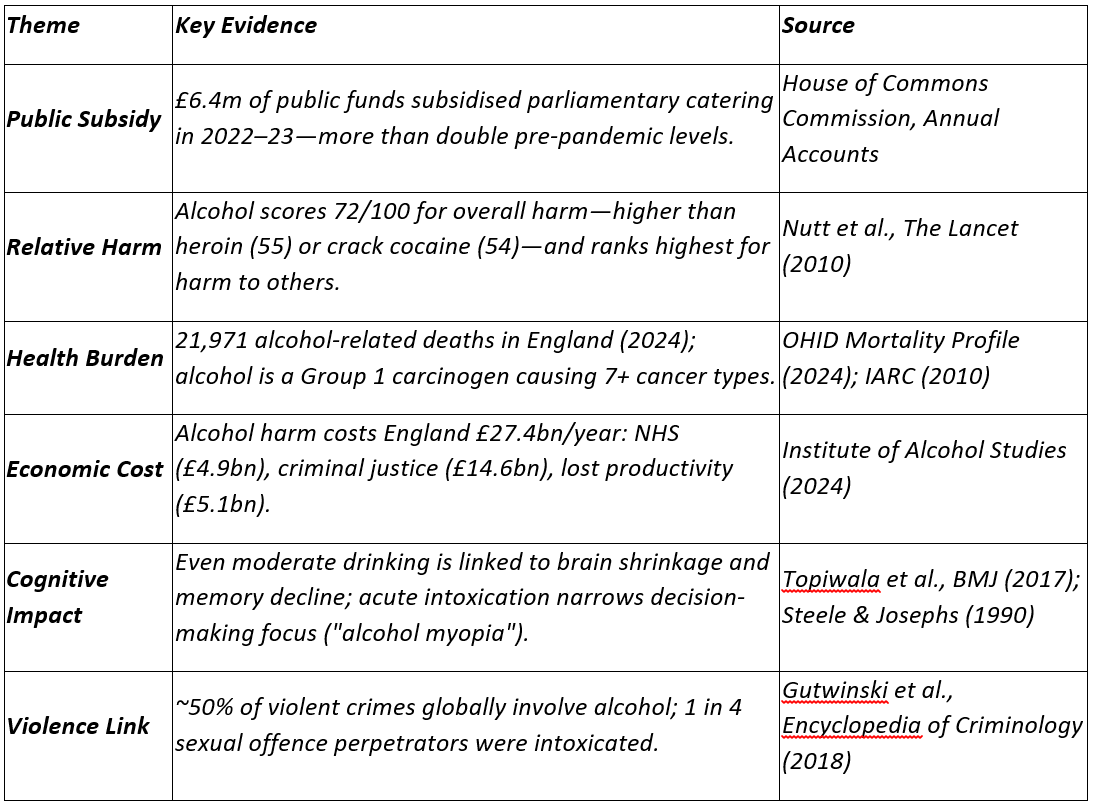
Contrary to occasional denials, the provision of food and drink in the Houses of Parliament operates at a structural financial loss that is offset by the state. Accounts from 2022–23 show that the public purse contributed £6.4 million to effectively subsidise catering, a cost that, while down from a pandemic-era peak of £9.1 million, remains starkly above pre-2020 levels of £2.6 million. This fiscal plumbing allows for an environment where a pint of Carlsberg lager can be purchased for just £3.56, and a large glass of wine for little over £4.00—prices that have been noted to appear “stuck in time” and entirely decoupled from the economic reality facing the nation’s pubs.
This is not a marginal perk. Parliamentary authorities withheld details under transparency exemptions of reports detailing the scale of alcohol-related problems on the estate, figures obtained under the Freedom of Information Act revealed that in a single twelve-month period, more than 65,770 alcoholic drinks were sold in subsidised parliamentary bars. It is a volume that raises urgent questions about a workplace where decisions of war, welfare, and economic survival are made.
The Pharmacological Reality: Alcohol as the Most Harmful Drug
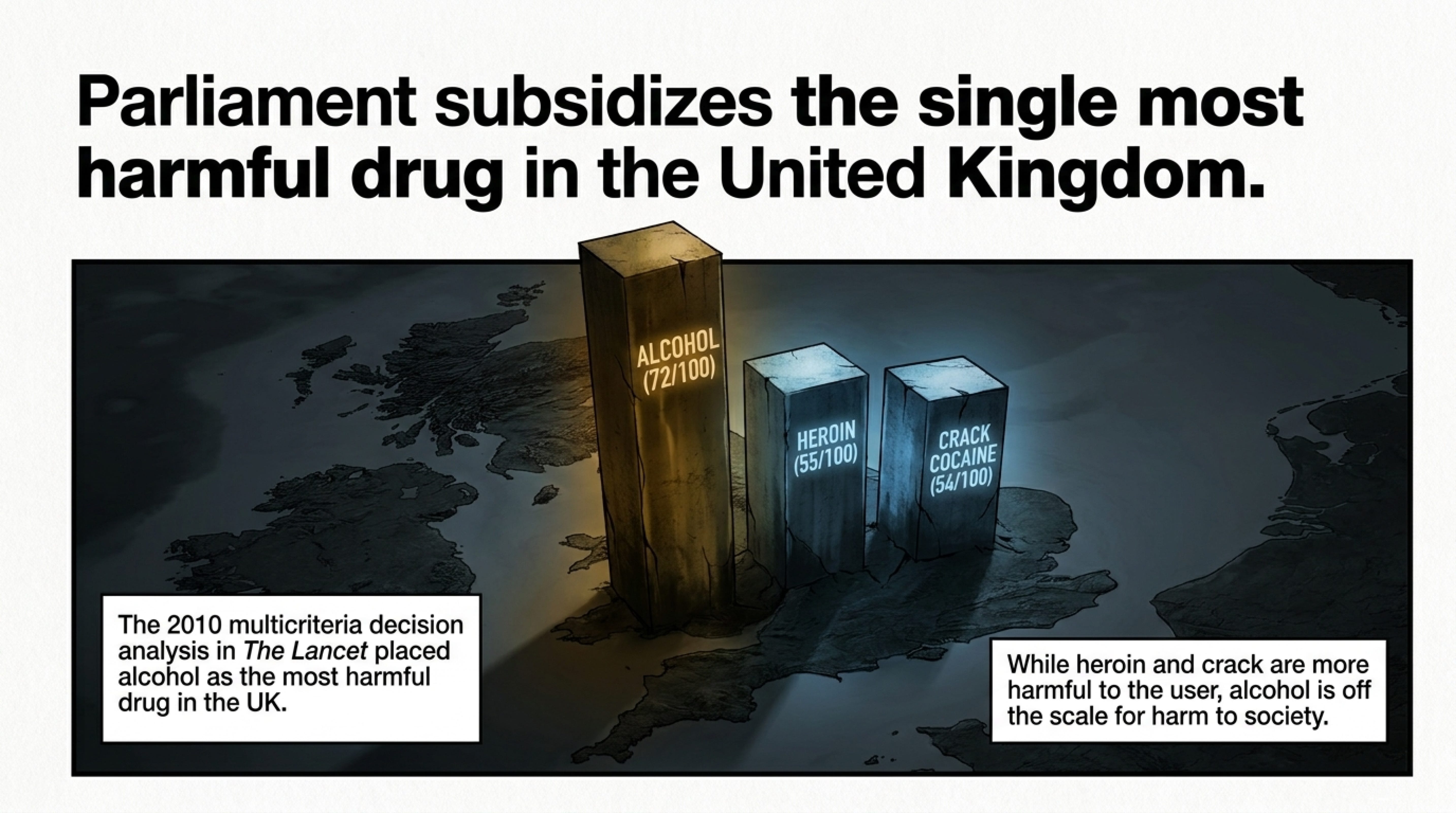
The clinical evidence for alcohol’s unprecedented capacity for harm is unequivocal. While politicians often grandstand on the war against illegal narcotics, landmark epidemiological work, notably the 2010 multicriteria decision analysis published in The Lancet, places alcohol in a category of its own. Using a framework that scored substances on sixteen criteria of harm—ranging from mortality and injury to family breakdown and economic cost—researchers found that alcohol was the most harmful drug in the United Kingdom, with an overall harm score of 72 out of 100. This placed it significantly ahead of heroin (55) and crack cocaine (54).
Crucially, where heroin and crack scored highly for harm to the individual user, alcohol was off the scale in terms of harm to others, scoring 46, compared to heroin’s 21. This distinction is critical; alcohol’s toxicity spills outwards, saturating public services, filling emergency rooms, and dismantling social cohesion.
A Tidal Wave of Mortality and Disease
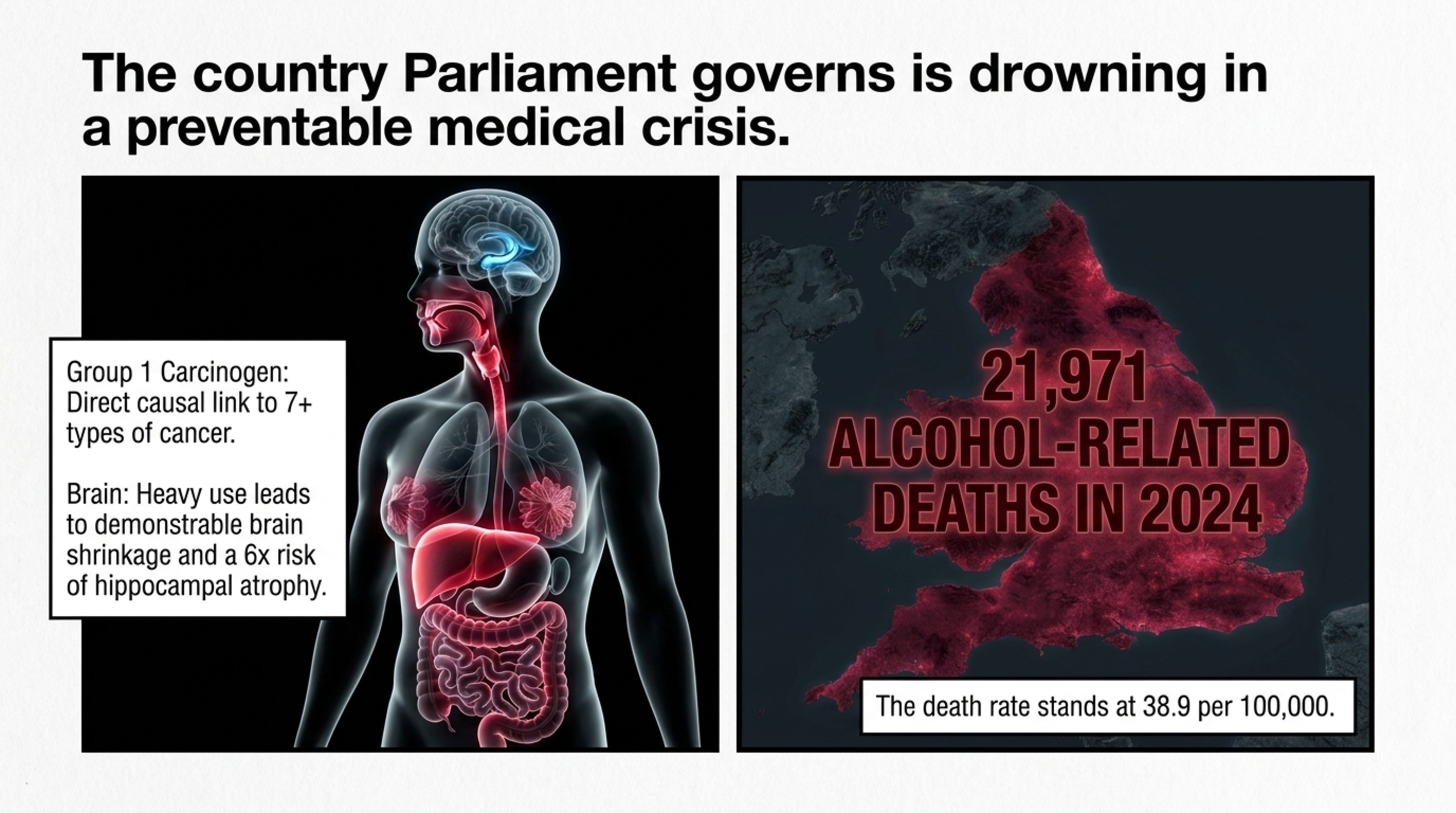
Parliament’s cheap pints exist within a country drowning in alcohol. The most recent 2024 mortality data from the Office for Health Improvement and Disparities reveals a bleak national picture: 21,971 people died from alcohol-related causes, with 7,763 of those deaths caused exclusively by alcohol (e.g., from alcoholic liver disease). This translates to an alcohol-related death rate of 38.9 per 100,000 people. The economic cost of this scale of harm is catastrophic. Researchers at the Institute of Alcohol Studies have calculated that alcohol harm costs England £27.4 billion annually. This figure includes £4.91 billion in direct NHS costs and a staggering £14.58 billion bled into the criminal justice system.
The long-term physiological consequences are often minimised in a culture that frames drinking as stress relief. Yet, the evidence is damning. Recent public health advisories confirm alcohol as a Group 1 carcinogen, with a direct causal link to at least seven types of cancer, including breast, bowel, and liver cancer. Neurologically, heavy habitual use leads to demonstrable brain shrinkage, with a BMJ study indicating that those consuming more than four drinks per day exhibited a sixfold increased risk of hippocampal atrophy—the erosion of the brain’s memory centre—compared to non-drinkers. This is compounded by alcohol’s established role in accelerating cognitive decline and the onset of dementia, with research confirming the direct neurotoxic effects of its metabolite, acetaldehyde.
The Alcoholic Fog in the Voting Lobby
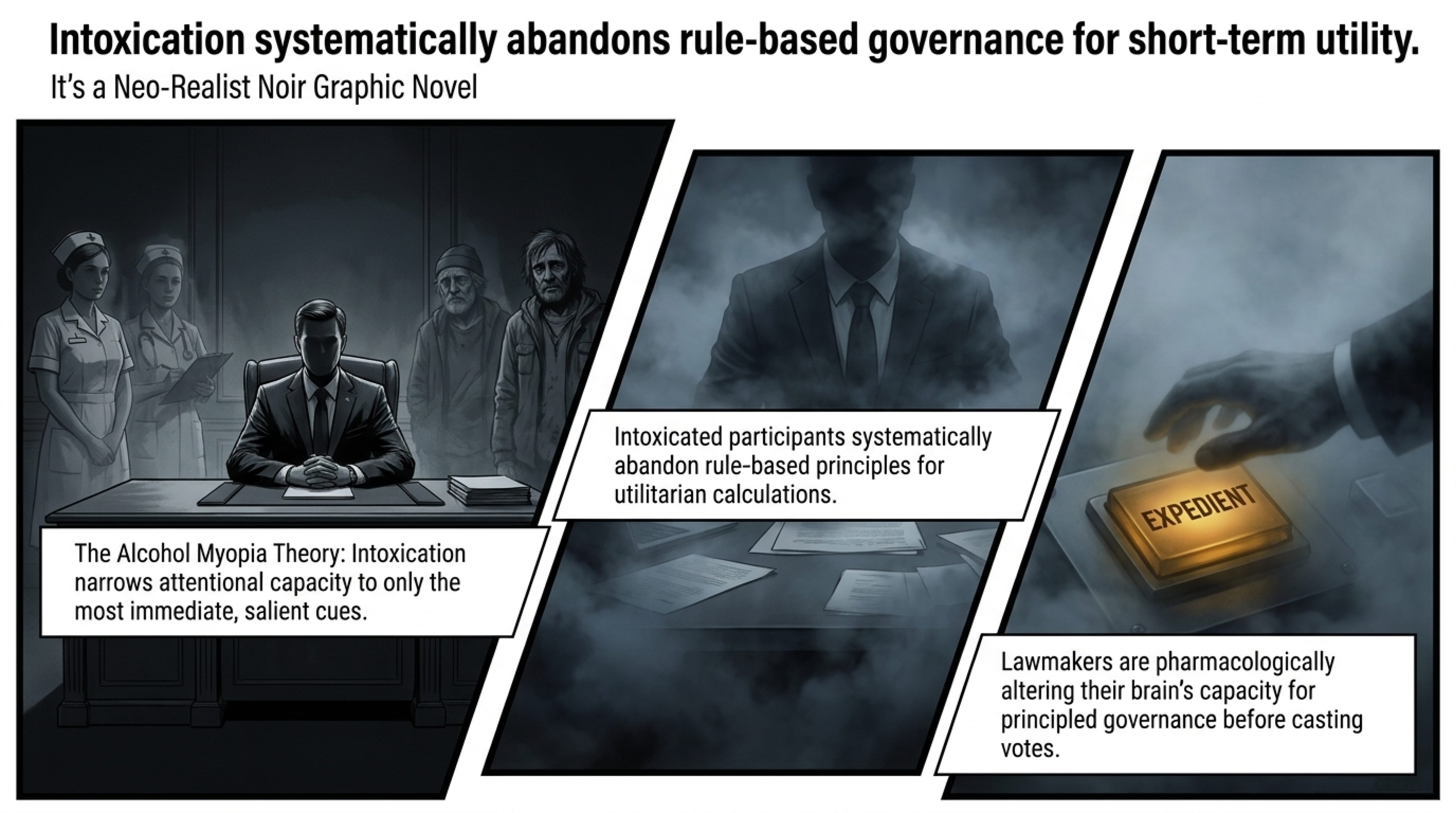
The physical dangers of cancer and cirrhosis, however grave, develop over decades. More immediately threatening to a legislature is alcohol’s capacity to highjack the moral and cognitive apparatus required to govern. The Alcohol Myopia Theory, a well-supported model in behavioural pharmacology, posits that acute intoxication narrows attentional capacity, forcing the inebriated brain into a state of cognitive short-sightedness where it reacts only to the most salient and immediate cues while neglecting complex, long-term consequences.
A rigorous 2022 pharmacological study published in Neuropsychopharmacology provided experimental evidence for this phenomenon. In a randomised placebo-controlled trial, researchers administered a moderate dose of alcohol (0.6 g/kg) to healthy adults. The result was a selective and significant shift in ethical decision-making: intoxicated participants systematically abandoned deontological (rule-based) principles in favour of utilitarian calculations. While no study has tested sitting MPs directly, the cognitive mechanics are well-established in controlled trials. In a political context, this suggests that a parliamentarian who pops into Strangers’ Bar for a subsidised glass of Sauvignon Blanc before a knife-edge vote is not simply relaxing—they are pharmacologically altering their brain’s capacity for principled, consistent judgment. They are rendering themselves more likely to make expedient decisions rather than right ones.
The psychiatric ramifications are equally severe. Chronic alcohol misuse is the second most commonly diagnosed cause of suicide, implicated in 15–43% of cases. Mental health services are left to pick up the pieces of a drinking culture that drives depression and anxiety, yet the very seat of legislative power remains a space where consumption is institutionally encouraged.
Violence, Impulsivity, and the Strangers’ Bar Brawl
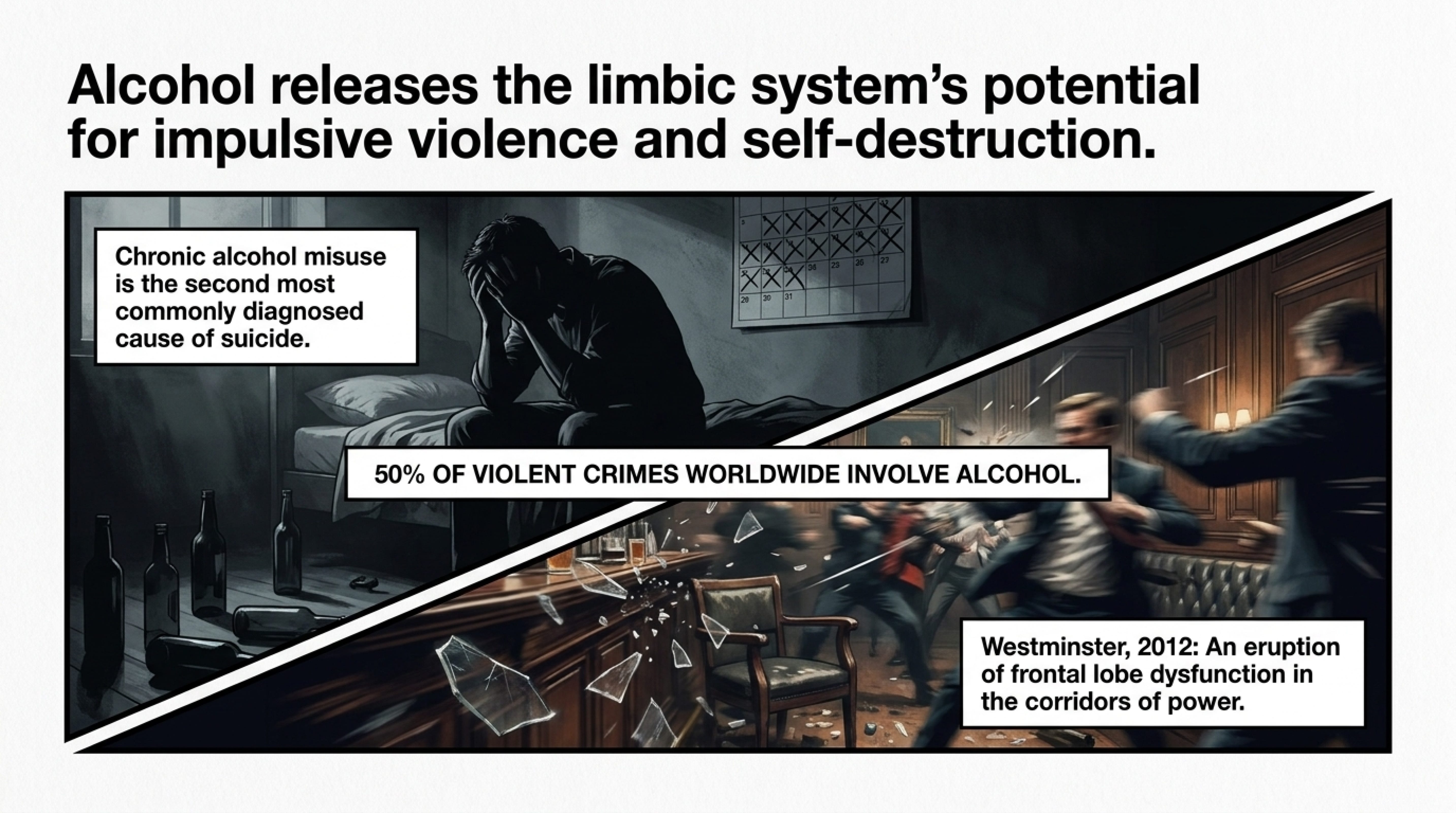
Alcohol’s propensity to ignite aggression is a deep-seated neurobiological fact. By dampening the function of the prefrontal cortex—the region responsible for inhibitory control—alcohol releases the limbic system’s potential for impulsive violence. Epidemiological data consistently show that acute alcohol intoxication plays a decisive role in approximately half of all violent crimes globally, including sexual assaults. In Germany, a country with comparable data tracking, nearly one in three solved violent crimes is committed under the influence (BKA annual crime statistics, 2023).
Nowhere is this link more physically apparent at Westminster than in the 2012 incident involving former Labour MP Eric Joyce, who was convicted of assaulting two Conservative politicians in a head-butting brawl inside the Strangers’ Bar. It was an eruption of frontal lobe dysfunction in the very corridors of power, and one that was managed not with a wholesale review of the culture, but with the Commons Speaker subsequently deploying Section 36 of the Freedom of Information Act to prevent the release of health reports specifically detailing the extent of parliamentary boozing.
The Sociological Entitlement of ‘One Law for Them’
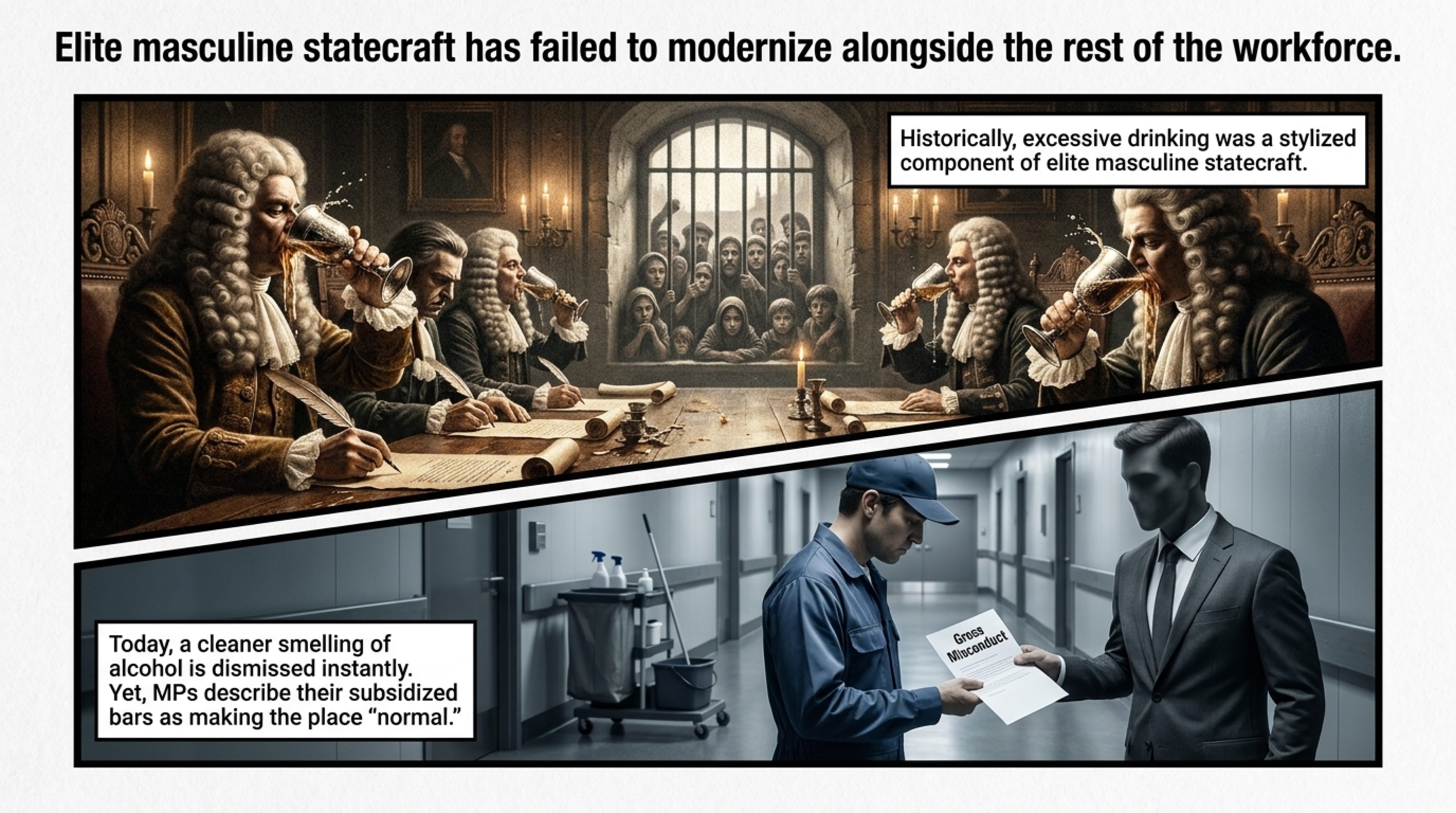
Why is this behaviour tolerated? The answer lies deep in the history of elite identity. As scholar Phil Withington has documented, from the seventeenth century onwards, excessive drinking was not merely a vice of the poor but a central, stylised component of elite masculine statecraft. The very architectural layout of Westminster—home to multiple subsidised bars—reflects a continuity of a pre-modern attitude in which “gentlemen” defined their own standards of civility while moralising against the intoxications of the lower classes.
This historical legacy manifests today as a staggering double standard. A cleaner or a bank clerk returning to their workplace smelling of alcohol would face gross misconduct proceedings. Yet, when the Green MP highlighted this precise discrepancy, Labour and Reform MPs dismissed her concern as “clickbait farming,” arguing that MPs are “human and sometimes have a drink”. This defence profoundly misrepresents the criticism: a relaxing evening pint is entirely different from a pervasive, subsidised drinking culture that operates during working hours in a safety-critical national workplace. It is a sense of absolution—a self-granted immunity from the norms of conduct their own legislation imposes on teachers, soldiers, and nurses.
The Double Standard of the Two Drugs
There is a glaring dissonance in the moral architecture of Westminster. The very parliamentarians who have belittled calls to address alcohol in the workplace—characterising them as “clickbait” and insisting that “MPs are human and sometimes have a drink”—are often the most vociferous in maintaining a punitive criminal justice approach for other substances. Reform UK leader Nigel Farage captured the prevailing attitude when he challenged the Green Party, asking how they could be “happy to legalise heroin and crack” yet think “an afternoon pint is a step too far”.
The implication is clear: in Westminster, alcohol holds a privileged and protected status, while the substances more commonly associated with poverty and social marginalisation are met with the full force of the law. The sheer cognitive dissonance of this arrangement—defending the right to be impaired at work while simultaneously legislating to incarcerate others for using different intoxicants—is staggering.
Yet this defence of alcohol’s special status sits uneasily with an overwhelming body of international evidence. The Green Party’s proposal to treat all drug use as a health issue rather than a criminal one draws directly on this evidence, distilling decades of research into a simple principle: the criminalisation of people who use drugs has been a catastrophic public health failure. The Johns Hopkins–Lancet Commission on drug policy and health found no evidence that the threat of imprisonment acts as an effective deterrent against drug use. Instead, criminalisation has actively worsened outcomes—incarceration reduces access to care, increases the risk of homelessness upon release, and creates prison environments where the absence of safe injecting equipment drives viral hepatitis and HIV transmission to levels approximately 35 times higher among people who inject drugs than in the general population.
This is not a marginal opinion. The United Nations has recognised the criminalisation of drugs as “proven to have negative health outcomes” and to “counter established public health evidence”. The weight of international consensus is that punitive drug laws drive stigma, push people away from health services, and increase unsafe practices—all factors that disproportionately harm already vulnerable populations.
Portugal provides the most cited real-world laboratory. When the country decriminalised the possession of all drugs for personal use in 2001, shifting from a punitive model to a public health approach, it did not see any increase in drug use or drug trafficking—a fact confirmed by senior Portuguese police officers. Instead, drug-related deaths declined, new HIV infections fell sharply, and the prison population for drug offences dropped from over 40% to under 16%. Treatment and harm reduction were scaled up dramatically. As the superintendent of Porto’s municipal police told an Irish parliamentary committee, decriminalisation proved an “outstanding” success—and critically, it required a generation of police to change their mindset from criminalising users to helping them.
The contrast could not be sharper. In Westminster, alcohol is treated as an entitlement—subsidised, normalised, and defended—while for the rest of society, particularly the poorest, drug use is met with the criminal law. The same parliamentarians who inhabit a workplace culture that normalises drinking during parliamentary hours preside over a system that imposes criminal sanctions on others for using substances that, in many cases, are far less physically and socially harmful than the alcohol they themselves consume.
The evidence shows, over and over, that a criminal justice approach does not reduce drug use but deepens the harms associated with it. By contrast, the health-led approach advocated by the Green Party—and adopted with documented success in multiple jurisdictions—aligns with both the scientific consensus and the stated positions of UN bodies.
A Global Productivity Crisis Mirrored at the Top
The economic argument against this culture makes the social argument irreversible. The Institute of Alcohol Studies found that alcohol-related productivity losses in the UK exceed £7.3 billion annually, with workplace hangovers alone costing £1.2–£1.4 billion per year in lost output. Corporate research demonstrates that a pervasive alcohol culture within an institution is negatively associated with employee treatment, sharpening management’s aggressive risk-taking while eroding protections for vulnerable staff. When the very people charged with maximising national productivity are themselves operating within an alcoholic haze of entitlement, the damage is not merely philosophical but measurable in lost GDP and blunted national competitiveness. The UK’s alcohol-related economic losses of £27.4 billion cast a long shadow over every parliamentary hour lost to hangovers and impaired judgment.
Time to Call Last Orders
The evidence gathered here is not a moralistic case against all public drinking. It is a clinical, criminological, and economic case against a specific, state-funded institutional exceptionalism that has outlived its time. Alcohol is the most physically damaging, socially corrosive, and cognitively disabling substance in the United Kingdom. For Parliament to continue to subsidise its consumption in the very heart of the legislature—while simultaneously hiding the evidence of its damage behind parliamentary privilege—is not merely hypocrisy. It is a dereliction of the duty of care owed to the public, and a legislative risk the country can no longer afford.
The Westminster bubble must align its behaviour with the laws, workplace standards, and medical realities it imposes on everyone else. The subsidy for alcohol in the Houses of Parliament should be withdrawn immediately.

If a surgeon cannot drink before an operation, a member of parliament should not drink before a vote.
It’s time to close the tab
This essay draws on peer-reviewed research from The Lancet, Neuropsychopharmacology, Deutsches Ärzteblatt, and reports from the Institute of Alcohol Studies, the Office for Health Improvement and Disparities, and Alcohol Change UK.
Reading List & Bibliography
This reading list curates the strongest available evidence on a question that sits at the intersection of public health, political culture, and social justice: Why does a society that criminalises some drugs continue to subsidise, normalise, and politically insulate the consumption of another—one that science ranks as the most harmful of all? The sources below move beyond opinion to document three interconnected realities: (1) the institutional structures that enable heavy drinking within Westminster; (2) the pharmacological and epidemiological evidence confirming alcohol’s exceptional toll on health, cognition, and public safety; and (3) the stark policy inconsistency that treats alcohol as a cultural commodity while punishing other substances with incarceration. This is not an argument for prohibition—it is a call for evidence-based consistency. If we accept that policy should follow science, then the current double standard demands urgent, honest re-examination.
One-Page Executive Summary: The Evidence in Brief
Core Findings
The scientific consensus is clear: alcohol causes exceptional, measurable harm to individuals and society. Yet UK policy treats it as a normalised commodity while criminalising other substances with lower evidence of harm. I hope that you will find that his reading list provides the evidence base to challenge that double standard.
The Institutional Framework: Subsidised Alcohol in Parliament
House of Commons Commission. Annual Report and Accounts (2020–2025). London: The Stationery Office.
https://www.parliament.uk/business/publications/
Official accounts showing £6.4m public subsidy for catering in 2022–23—down from £9.1m during the pandemic, but more than double pre-2020 levels.
Flinders, M. (2015). The politics of the Westminster village. Parliamentary Affairs, 68(Suppl 1), 98–115.
https://doi.org/10.1093/pa/gsv012
Academic analysis of Westminster’s insular culture—essential context for understanding why institutional drinking persists.
Grey, S. & Van Ommeren, E. (2020). Bars, booze and bills: alcohol cultures in parliaments. Journal of Legislative Studies, 26(3), 437–456.
https://doi.org/10.1080/13572334.2020.1779159
The only dedicated academic study of drinking cultures in legislatures—directly relevant to your thesis.
The Pharmacological Reality: Alcohol as the Most Harmful Drug
Nutt, D. J., King, L. A. & Phillips, L. D. (2010). Drug harms in the UK: a multicriteria decision analysis. The Lancet, 376(9752), 1558–1565.
https://doi.org/10.1016/S0140-6736(10)61462-6
Landmark study: alcohol scores 72/100 for overall harm—higher than heroin (55) or crack (54)—and highest for harm to others.
van Amsterdam, J. & van den Brink, W. (2010). Ranking of drugs: a more balanced risk-assessment. The Lancet, 376(9752), 1524–1525.
https://doi.org/10.1016/S0140-6736(10)62000-4
Expert commentary on the Nutt study—useful for anticipating methodological critiques.
Babor, T. F. et al. (2010). Alcohol: No Ordinary Commodity – Research and Public Policy (2nd ed.). Oxford University Press.
https://global.oup.com/academic/product/alcohol-no-ordinary-commodity-9780199551149
The definitive textbook on alcohol policy—authoritative, evidence-based, and widely cited by WHO and governments.
A Tidal Wave of Mortality and Disease
Office for Health Improvement and Disparities (OHID). (2024). Mortality Profile: Statistical Commentary, December 2024. London: DHSC.
https://www.gov.uk/government/collections/alcohol-profiles
Latest official data: 21,971 alcohol-related deaths in England (2024); rate of 38.9 per 100,000 population.
Institute of Alcohol Studies (IAS). (2024). The £27.4 billion cost of alcohol harm in England. London: IAS.
https://www.ias.org.uk/publications/the-27-4-billion-cost-of-alcohol-harm-in-england/
First comprehensive cost analysis in 20+ years: breaks down NHS, criminal justice, productivity, and social care burdens.
Bhattacharya, A. (2017). Splitting the bill: alcohol’s impact on the economy. Addiction, 112(Suppl 2), 58–65.
https://doi.org/10.1111/add.13822
Explains why calculating alcohol’s true cost is complex—important context for interpreting the £27.4bn figure.
International Agency for Research on Cancer (IARC). (2010). Alcohol Consumption and Ethyl Carbamate (Vol. 96). Lyon: IARC.
https://monographs.iarc.who.int/monographs/100E/
Confirms alcohol is a Group 1 carcinogen—causing 7+ cancer types, with no safe threshold.
Topiwala, A. et al. (2017). Moderate alcohol consumption and cognitive decline. The BMJ, 357, j2353.
https://doi.org/10.1136/bmj.j2353
Even “moderate” drinking linked to brain shrinkage and memory decline—challenges the “one glass is fine” narrative.
Rehm, J. et al. (2017). Alcohol use and burden of disease: an update. Addiction, 112(6), 968–1001.
https://doi.org/10.1111/add.13757
Global evidence review reinforcing alcohol’s causal role in disease, injury, and premature death.
The Alcoholic Fog in the Voting Lobby
Steele, C. M. & Josephs, R. A. (1990). Alcohol myopia: its prized and dangerous effects. American Psychologist, 45(8), 921–933.
https://doi.org/10.1037/0003-066X.45.8.921
Foundational theory: intoxication narrows focus to immediate cues, impairing long-term reasoning—highly relevant to legislative decisions.
Opitz, A. et al. (2022). Acute effects of alcohol on moral decision-making. Neuropsychopharmacology, 47, 824–831.
https://doi.org/10.1038/s41386-021-01218-9
Experimental study: moderate alcohol shifts moral judgments toward utilitarian (outcome-focused) choices—potential implications for policy votes.
Conner, K. R. & Bagge, C. L. (2019). Alcohol use and suicidal behaviour. Alcohol Research: Current Reviews, 40(1), arcr.v40.1.05.
https://doi.org/10.35946/arcr.v40.1.05
Meta-analysis confirming alcohol as a key risk factor for suicide—critical for understanding acute harm.
Violence, Impulsivity, and the Strangers’ Bar
Gutwinski, S., Heinz, A. & Schäfer, I. (2018). Alcohol-related violence. In Encyclopedia of Criminology and Criminal Justice. Springer.
https://doi.org/10.1007/978-1-4614-5690-2_1833
Global review: ~50% of violent crimes involve alcohol; 1 in 4 sexual offence perpetrators were intoxicated.
Miczek, K. A. et al. (2015). Neurobiology of escalated aggression. Journal of Neuroscience, 35(24), 8930–8943.
https://doi.org/10.1523/JNEUROSCI.0143-15.2015
Explains how alcohol impairs brain regions that regulate impulse control and aggression.
BBC News. (2012, February 23). Labour suspends MP Eric Joyce after Commons “assault”.
https://www.bbc.co.uk/news/uk-politics-17143215
Contemporary reporting of the 2012 Strangers’ Bar incident—useful for illustrating real-world consequences.
The Sociological Entitlement of “One Law for Them”
Withington, P. (2013). Intoxicants and the early modern state. The Historical Journal, 56(3), 631–655.
https://doi.org/10.1017/S0018246X13000211
Shows how heavy drinking was historically embedded in elite male governance—context for today’s parliamentary culture.
Greenfield, T. K. et al. (2011). Externalities from alcohol consumption. In Alcohol: Science, Policy and Public Health. Oxford UP.
https://doi.org/10.1093/acprof:oso/9780199551149.003.0025
Introduces “externalities” framework: helps explain the gap between private drinking pleasure and public harm.
The Double Standard: Alcohol vs. Illegal Drugs
Johns Hopkins–Lancet Commission. (2016). Public Health and International Drug Policy. The Lancet, 387(10026), 1427–1480.
https://doi.org/10.1016/S0140-6736(16)00601-X
Major commission: finds criminalisation worsens health outcomes and fails to deter use.
Hughes, C. E. & Stevens, A. (2010). What can we learn from Portugal’s decriminalisation? British Journal of Criminology, 50(6), 999–1022.
https://doi.org/10.1093/bjc/azq038
Seminal analysis: Portugal’s health-led approach reduced deaths, HIV, and incarceration—without increasing drug use.
Laqueur, H. (2015). Uses and abuses of drug decriminalization in Portugal. Law & Social Inquiry, 40(3), 746–769.
https://doi.org/10.1111/lsi.12111
Critical perspective: cautions against oversimplifying Portugal’s success—useful for nuanced argumentation.
Global Commission on Drug Policy. (2023). Decriminalisation of Drugs Will Reduce Public Health Threats. Geneva: GCDP.
https://globalcommissionondrugs.org/report/decriminalisation-will-reduce-public-health-threats/
Contemporary policy brief citing UN recognition that criminalisation contradicts public health evidence.
A Global Productivity Crisis Mirrored at the Top
Institute of Alcohol Studies (IAS). (2024). Alcohol Harm: A Hidden Productivity Crisis in the UK Workforce. London: IAS.
https://www.ias.org.uk/publications/alcohol-harm-a-hidden-productivity-crisis/
Finds £7.3bn+ annual productivity loss in UK; workplace hangovers cost £1.2–1.4bn alone.
Roche, A. M., Pidd, K. & Kostadinov, V. (2015). Alcohol and work: patterns, culture, safety. Safety Science, 79, 210–218.
https://doi.org/10.1016/j.ssci.2015.06.007
International review linking workplace drinking to accidents, absenteeism, and reduced output—parallels Westminster culture.
Foundational & Cross-Cutting Works
Babor, T. F. et al. (2010). Alcohol: No Ordinary Commodity (2nd ed.). Oxford University Press.
https://global.oup.com/academic/product/alcohol-no-ordinary-commodity-9780199551149
The single most comprehensive, evidence-based guide to alcohol policy—referenced throughout this list.
Room, R., Babor, T. & Rehm, J. (2005). Alcohol and public health. The Lancet, 365(9458), 519–530.
https://doi.org/10.1016/S0140-6736(05)17870-2
Concise, influential overview of alcohol’s global disease burden—ideal for readers new to the topic.
World Health Organization. (2018). Global Status Report on Alcohol and Health. Geneva: WHO.
https://www.who.int/publications/i/item/9789241565639
Authoritative international data—useful for comparing UK patterns with peer nations.